 ��ӡ����
��ӡ����  �رմ���
�رմ��� For around 200 years, two very different systems of medicine have been used in Asia to cure diseases and keep people healthy. The local Asian one is based on traditional Chinese medicine (TCM) �� herbal mixtures developed though observation and experience accumulated over thousands of years, but with unknown mechanisms of action. On the other hand, modern medicine, imported from the West, consists of chemically purified compounds that have been discovered through scientific investigation and tested in controlled clinical trials. They differ in the composition of their medicines, the process of diagnosis, methods of proving a treatment's effectiveness, and even in their concept of 'health' (see 'Made in China', page S82).
GRACIA LAM
Are these differences irreconcilable? Or, if TCM is modernized to the point where it can make scientifically valid claims, might it offer new perspectives that can benefit modern medicine �� including clues on how to tackle the least tractable diseases and conditions? And likewise, can new perspectives being advanced in the West, such as systems biology, help lay a scientific foundation for TCM?
Spirituality in medicine
Although modern medicine has its roots in herbalism and in ancient Greek traditions that share many similarities with TCM, the practice of medicine was transformed by the Enlightenment and the consequent revolution in science and technology. Since the late eighteenth century, Western-style medicine has incorporated knowledge of anatomy, physiology, chemistry and biology, and its methods are evidence-based. TCM, although it is starting to take on these attributes, still relies heavily on ancient records and traditional practices.
TCM includes many tenets derived from Taoism, Confucianism and ancient Indian philosophies that describe the natural world, life and the human body. Concepts include yin and yang, which represent opposing yet complementary essences of nature; wuxing, which covers the five basic elements of the universe (wood, fire, earth, metal and water); qi or energy; and xue, the blood. This terminology purports to be concerned with disease and human health, but cannot be defined in terms of biochemical or biological facts �� or indeed measured. And even the literal translation of these tenets into other languages is misleading.
The modern medical and scientific communities in China and elsewhere are highly critical of such mystical concepts, which are consequently becoming marginalized in China. ��The medical practice of TCM is a process of trial and error, and concerns the understanding and control of herbs from the Chinese Materia Medica,�� says Daqing Zhang, director of the Center for History of Medicine at Peking University in Beijing. ��The philosophical theories were created afterwards to provide the explanatory framework for the practices, and are used to win the patients' trust.��
But thousands of years of history is a long time to cement a belief, and the theories of TCM still have their firm defenders, such as Boli Zhang, president of the China Academy of Chinese Medical Sciences (CACMS) in Beijing. ��We believe in the jing luo [the meridian or energy pathways], but we have not found it yet,�� he says. Nevertheless, even in the TCM community, there are fewer Chinese scholars who believe the TCM tenets literally. Indeed, there has been criticism from academics and the media in China, arguing that much of TCM and most of its theories are pseudoscience and that China should bid ��farewell to traditional Chinese medicine��1.
Despite these negative sentiments, the Chinese government has started to promote TCM by allocating large funds for research (see 'One step at a time', page S90). Influential figures in the TCM community, such as Boli Zhang and his deputy Baoyan Liu at CACMS, are pushing for the modernization of TCM while also emphasizing its unique qualities. These advocates insist that the traditional TCM practices should be preserved for as long as possible to better investigate their heritage. ��The advantages and disadvantages of the two systems are the premise of the integration,�� says Liu.
Closing the gaps
One practice in TCM that is adapting to science is diagnosis. Each patient receives a personal diagnosis based on a TCM syndrome or zheng, which is a characteristic phenotype of identifiable manifestations gleaned from general appearance, listening to and smelling the patient, feeling the pulse and asking questions. TCM diagnosis includes many symptoms considered less important in modern medicine, such as thirst, the tongue's condition, whether the limbs feel cold, and mood. In contrast, modern disease diagnosis is based primarily on clinical signs such as temperature and blood pressure, pathological examination of individual organ functions and biochemical analysis of blood or urine.
��Chinese herbal medicine identifies and treats syndromes rather than diagnosed diseases,�� explains Aiping Lu, director of the Institute of Basic Research in Clinical Medicine at CACMS. TCM syndromes are a finer level of classification than disease groupings in modern medicine. Lu's group is collaborating with several Western research institutes on rheumatoid arthritis. In one study, his team used 18 different clinical TCM signs to classify rheumatoid arthritis patients into four subgroups, corresponding to presence of joint symptoms (tenderness, swelling and stiffness), cold pattern (joints and limbs feel cold to the touch, and patient is intolerant of cold), deficiency pattern (including weakness, dizziness, fatigue and nocturia) and hot pattern (including joints that feel hot, vexation, fever and thirst). Then all patients were randomized to receive either modern medicine or a TCM treatment. Each TCM-defined sub-group responded differently to treatment. ��The results show TCM syndromes improved the efficacy of both TCM and modern medicine interventions,�� says Lu. Notably, patients with cold-pattern symptoms responded better to modern medicine, whereas those classified with a deficiency pattern benefited most from a TCM intervention2. The next step is to analyse the patients' metabolites to look for underlying biochemical differences between the different TCM syndromes, to see if there is a link between TCM diagnoses and modern medical definitions (see 'All systems go', page S87).
The composition of TCM medications is at odds with modern medicine too. TCM uses compound formulae (fufang) that contain several herbs thought to act in unison to restore what TCM practitioners call the patient's 'balance'. ��It is an advantage of TCM that multiple drug components can strengthen the therapeutic efficacy and attenuate the toxicity of major component(s) through drug�Cdrug interaction in vivo,�� says Wei Jia, co-director of the Center for Research Excellence in Bioactive Food Components at the University of North Carolina at Greensboro.
Another advantage of a formula that acts on several fronts is that each ingredient does not have to be so potent. ��If we use medium-active ingredients, which comprise the majority of compounds in nature, we have more potential drug candidates, achieve weaker side effects and have lower R&D costs,�� says Zhimin Wang, a chemist at CACMS' Institute of Chinese Materia Medica.
TCM practitioners formulate their herbal remedies according to a set of principles (peiwu), which organize ingredients in any fufang into four functional roles: sovereign, minister, assistant and envoy. The sovereign is the ingredient with major pharmacological activity. The ministers provide additive or synergistic activities. Assistants can either augment the pharmacological effect, detoxify or even counteract an excessively strong action. Envoys harmonize the whole recipe to ensure that all the substances in the fufang are compatible.
There is early evidence supporting the peiwu principles. A team led by molecular biologists Zhu Chen and Saijuan Chen at Jiao Tong University in Shanghai analysed the Realgar�CIndigo naturalis formula �� a TCM-based leukaemia treatment containing realgar, indigo minerals and the herb red sage root (danshen). They found that the arsenic in realgar could be described as the 'sovereign' as it attacked the main oncoprotein in leukaemia cells; indirubin, the active ingredient in indigo, worked as the 'assistant' to slow leukaemia cell growth; and tanshinone, from red sage root, served as 'minister' to help restore the damaged pathways that prevent leukaemia spreading. Indurbin and tanshinone also worked as 'envoys' to enhance cellular uptake of arsenic3.
��A TCM formula is structural, and using the ingredients should be like a military operation,�� says Zhong Wang, a professor at CACMS' Institute of Basic Research in Clinical Medicine, who has developed a concept that covers the science of TCM formulae �� fangjiomics4. Fangjiomics separates biological networks into discrete, interactive modules that can be targeted separately but whose biological effect must be considered together. Zhong Wang argues that, compared with the Western model of single-target interventions, TCM combinations are systematic and well ordered.
The long way ahead
��Could Western treatments of chronic diseases be improved by insights from TCM?��
The triumphs of modern medicine in the past 200 years have been most striking in preventing and curing infections and acute disease, and in pain relief. By contrast, progress in understanding and treatment of chronic and degenerative diseases has been slow. And it is these conditions, such as diabetes and Alzheimer's disease, that are responsible for a large portion of the West's soaring and unsustainable healthcare costs. Could Western treatments of these diseases, where there is no infectious agent but rather an internal imbalance in the immune system or other biological housekeeping systems, be improved by insights from TCM?
In modern medicine, chronic conditions are generally treated with prolonged administration of chemical drugs, which can give rise to long-term toxicity or even resistance. That's what happens, for example, with many patients taking isosorbide dinitrate for chronic angina pectoris. The danshen dripping pill provides a better long-term curative effect, claims Jia. As it contains a mixture of ingredients, each individual component can be added at a lower, less-potent dose without compromising the effectiveness of the overall preparation. Moreover, TCM preparations tend to be cheaper than modern pharmaceuticals, he adds.
In addition to being a source of national and cultural pride, Chinese herbal medicines are the most promising source of new drugs for the Chinese pharmaceutical industry, which has always lived in the shadow of Western pharmaceutical giants. China is stepping up its efforts in both academia and the pharmaceutical industry to find safe and effective compound formulae that are acceptable to Western regulatory agencies. Most attempts have focused on isolating a single active ingredient from the TCM preparations. This reductionist, Western approach has led to only a few successes �� including the antimalarial drug artemisinin and the leukaemia treatment arsenic trioxide.
So far, no drugs based on established TCM formulae have been approved in the United States or Europe. The nearest example is sinecatechins (marketed as Veregen by German biotech MediGene based in Martinsried), a cream made from a mixture of green tea extracts for the treatment of genital and perianal warts. Sinecatechins was approved in 2006 by the US Food and Drug Administration, and is the FDA's first and only 'botanical' drug �� approved on clinical results despite the fact that the active ingredients and the mechanism of action are not known (see 'Herbal medicine rule book', page S98). However, the danshen dripping pill, manufactured by the Tainjin-based Tasly Group in China, has successfully completed phase II trials in the United States and could be the first botanical drug derived from the TCM repertoire.
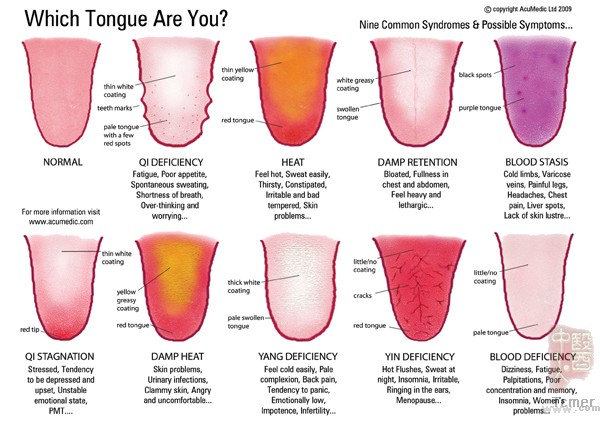
ACUMEDIC LTD (2009)
��Pharmaceutical regulations in the West are developed according to the Western way of drug R&D, and they are not fit for evaluating TCM drugs,�� says Henry Sun, vice-president of Tasly Group. ��Of course, TCM should be proved on the basis of scientific evidence.�� However, Sun argues that the science is skewed towards testing single agents targeted to single mechanisms (see 'The clinical trial barriers', page S93). ��Besides the science, the other major challenge is convincing different groups in the West, from ordinary people to policymakers, to change their prejudices against TCM.��
Top down or bottom up?
The advent of �Comics technologies that rapidly measure the entirety of the human complement of, for example, genes (genomics) or metabolites (metabonomics) �� and to integrate these diverse data into a complete picture �� has given rise to a new way of looking at medicine in the form of systems biology. For many TCM researchers, such as Aiping Lu and Zhong Wang, systems biology is potentially a way to understand TCM using Western scientific methodology.
��The major challenge of the integration of TCM and modern medicine is the translation from TCM experience and concepts into biochemical and biological meanings that Western scientists can understand,�� says Jan van der Greef, a systems biologist at Leiden University in the Netherlands. ��Systems biology is an ideal theory and analysis tool that can bridge the two systems.��
Leroy Hood, president of the Institute for Systems Biology in Seattle, Washington, and regarded by many as the field's founding father, has introduced what he calls '4P healthcare': predictive, personalized, preventive and participatory. This concept, Hood contends, is the new paradigm of modern medicine in a systems biology era. 4P medicine focuses on the biochemical networks underlying health and disease, then aims to treat and prevent disease by identifying and countering perturbations in the biological networks �� a concept highly reminiscent of the TCM philosophy. Thanks to systems biology, the gap between the two medical systems is starting to narrow. For example, recent advances in medical technology are allowing the application of new phenotyping technologies that can simultaneously characterize the multiple drug responses to dietary preparations, such as pu-erh tea. In a proof-of-concept study in humans, a team led by Jia quantitatively measured the absorption of pu-erh tea molecules, the output of gut bacteria metabolism, and the human metabolic response profile in the urine5. ��The phenotyping strategy can further differentiate disease subtypes that are correlated to different TCM syndromes,�� says Jia. This, in turn, will ��improve doctors' ability to personalize treatment and to predict an individual's response to a drug regimen��.
But Jia and others are aware that the technology and methodology of systems biology are still immature. ��We have to first develop network models to simulate a pathogenesis: for example, the transformation of normal cells to cancer cells,�� says Jia. ��The second step will be to model a multi-component agent targeting the multiple sites involved in the transformation process.��
East meets West
The absence of scientific development processes and controlled clinical trials has held back the integration of traditional Asian medicine and modern medicine for centuries. Some of its concepts appear more magical than practical, and, without a physical basis, have resisted measurement and observation. But slowly these differences are resolving.
Much of the drive for integration will come from China and its neighbours. ��We should build our own methodology to evaluate the unique features and efficacy of TCM,�� says Zhimin Wang. ��There are so many possible ways of integration between TCM and modern medicine. We should keep our minds open.��
The days of competition between these two systems could well be gone. ��The two systems cannot replace each other,�� says Boli Zhang. ��But instead they will fill each other out.��
Convergence: Where West meets East
Peng Tian
Nature Volume: 480, Pages: S84�CS86 Date published: (22 December 2011)
doi:10.1038/480S84a
Published online 21 December 2011
http://www.nature.com/nature/journal/v480/n7378_supp/full/480S84a.html
200�������������dz���ͬ��ҽѧϵͳһֱ�����������ţ����Ƽ�������֤����Ľ��������ޱ�����ҽ�ƻ�����ҽ���ۺ���ҩ��������ͨ����ǧ��Ĺ۲�;�����۷�չ�����IJݱ�ҩ��Ļ�������֪�����û���������һ�������ִ�ҽѧ�����������ڵģ��ɾ���ѧ�о����ֲ�ͨ�����Ƶ��ٴ�������Թ��Ļ�ѧ�ᴿ��������ɡ�������ҩ����ɣ���Ϲ��̣�֤�������ֶ���Ч�ķ����������ڽ����Ŀ����϶����Ų��졣
��Щ�����Dz��ɵ��͵��𣿻���˵�������ҽ�ܹ���һЩ�ؼ��������п�ѧ���ݵ��۶ϣ�Ҳ���ܹ�����µ��������ִ�ҽѧ�Ĺ۵㡪����������ȥ������ֵļ����������һЩ��ʾ��ͬ���أ����������һЩ�¹۵㣬����ϵͳ����ѧ���Ƿ��ܹ�������ҽ����һ����ѧ�Ļ�����
ҽѧ�ľ���
��Ȼ�ִ�ҽѧ�����ڱ���ҽѧ�ϣ����ҹ�ϣ����ͳҽѧ���й���ͳҽѧ������������֮����������ҽѧ��ʵ�����������������˶������ĿƼ����¶������˸ı䡣��ʮ����������������ģʽ��ҽѧ�ɽ���ѧ������ѧ����ѧ������ѧ��֪ʶ�������ɣ������ķ����Ǹ���֤�ݵġ���ҽ����Ȼ��ʼ�Ӵ���Щ����������Ȼ�Ƿdz������ڹŴ�������¼�ʹ�ͳ��ʵ��������
��ҽ��������Դ�Ե��ҡ���Һ�ӡ����ѧ��������Ȼ���硢�����������ԭ����������Yin����Yang�ĸ����������Ȼ���������ı��ʣ�����Wuxing����������������ֻ���Ҫ�أ�ľ�����������ˮ������Qi������˵����������Ѫxue����ѪҺ����Щ�����Ǿ����彡���ͼ������Եģ����Dz��������ﻯѧ������ѧ�ϵĿ���ʵ�����壬����ʵ�������������ġ���������Щԭ��ֱ����������Ծͻ�������⡣
���й��������ط����ִ�ҽѧ�Ϳ�ѧ�������Щ���صĹ�����������ɣ����������й���Щ˼����ų�ͺ��ӡ�����ҽ��ҽ��ʵ����һ����������Ĺ��̣��漰���������Ϳ���ʹ���в�ҩ����������ѧҽѧʷ���������Ŵ���˵����������һЩ��ѧ����Ϊ��Щҽ��ʵ���ṩһ��˵���Ŀ�ܣ�������ȡ�ò��˵����Ρ���
������ǧ�����ʷ����Щ�������㹻����ʱ��ȥ���̣�������ҽ��������Ȼ������ʵ�ĺ����ߣ������Ų������й���ҽ��ѧԺԺ�������������ž���[�����������������ͨ��]�Ĵ��ڣ��������ǻ�û���ҵ���������˵����Ȼ��ˣ���ʹ����ҽ�磬������ҽ���۵��й�ѧ��Խ��Խ�١�ʵ���ϣ����й���ѧ�����ý�嶼����ҽ���������У���Ϊ��ҽ������ط������ľ������۶���α��ѧ���й�Ӧ�ñ�ʾ����ҽ˵�ټ���
�����кฺܶ��Ŀ������й�������ͨ���������о��ʽ���֧����ҽ����ҽ����Ӱ�������ˣ������й���ҽ��ѧԺ���Ų�����Ժ�������ӣ����ƶ���ҽ�ִ����Ĺ�����ͬʱǿ��������ԡ���Щӵ�������ΪӦ�����ܵر�����ҽ��ͳҽ��ʵ�����������Ӷ����õؼ̳���Щ�Ų�������������ҽ��ϵͳ���ŵ��ȱ�����������ϵ�ǰ�ᡣ��������˵��
���϶
ʹ��ҽ��Ӧ��ѧ��һ����������ϡ�ÿһ�����˶���������ҽ�ϵġ�֢�����õ����˵���ϵġ���֢����һЩͨ���������е����Ŀ�ʶ��ĵ��͵��ٴ�֢״����ҽ�ϵ�����֢״���ִ�ҽѧ�������Ǻ���Ҫ������ڿʣ���ͷ���������֫�Ƿ���Ͳ��˵����������ִ��ļ����������Ҫ�����ٴ���֢״�������¡�Ѫѹ���������ٹ��ܵIJ���ѧ����Լ�ѪҺ����Һ������������
���в�ҩ����ʱ���Ƕ�֢�����ǶԲ���������ƽ���ͣ������й���ҽ��ѧԺ��ҽ�ٴ�ҽѧ�����о���������������ҽ��֢������ִ�ҽѧ�ļ������෨���ԣ���һ�ָ��õķ��ʽ�������Ŷ����ͼ��������о���չ����ʪ�Թؽ�����ĺ�������һ���о��У������ŶӸ���18����ͬ����ҽ֢��ѷ�ʪ�Թؽ��ײ��˻��ֳ��ĸ����飬�ֱ��ǹؽ�֢״�飨ѹʹ�����ͺͽ�Ӳ�������飨�ؽں���֫����ȥ���䣬���Ҳ����������ܺ��䣩�����飨����������ͷ�Σ�ƣ�ͺ��������飨�����ؽڷ��ȡ����ꡢ���պͿڿʣ���Ȼ�����еIJ��˶��������ִ�ҽѧ������ҽ�����ơ�ÿһ������ҽ���������ʹ�����Ӧ�����Ʒ������������ʾ��ҽ֢��ͬʱ�ٽ����ִ�ҽѧ����ҽ����Ч������˵���ر��ǹ�Ϊ����IJ��˶��ִ�ҽѧ�����Ʒ�Ӧ���ã�����Щ����Ϊ����IJ��˶���ҽ�����Ʒ�Ӧ��ѡ���һ����Ҫ�������˵Ĵ�л������ò�ͬ����ҽ֢��֮��DZ�ڵ��������죬�Ӷ���ȷ��ҽ����Ϻ��ִ�ҽѧ������֮���Ƿ�������ϵ��
��ҽ��ҩ�����Ҳ���ִ�ҽѧ��ͬ����ҽʹ���ɼ��ֲ�ҩ���ɵĸ���ͬʱ����������ȥ�ָ���ҽʦ��ν�IJ��˵�ƽ�⡣��ͨ��ҩ���ҩ��֮�������ڵĻ��������ö���ҩ��ɷ�����ǿ��Ч��������Ҫ�ɷֵĶ������ã�������ҽ���ŵ㡣�����������������ݴ�ѧʳ��������Գɷ�Խ�о����ĵ���������Wei Jia˵��
���������ŵ�֮�⣬���������ƻ����ڲ���Ҫÿһ���ɷֶ���ǿ��Ч�ġ����������ʹ�ô������Ч�ɷ֣����а�����Ȼ���ɵĴֻ������ô���ǽ��и��������Ч��ҩ���������壬���Ҹ����ø��ͣ��з��ɱ�Ҳ���١����й���ҽ��ѧԺ��ҩѧ�о�����ҩ��ʦZhimin Wang˵��
��ҽʦ����һЩ����ԭ����������ǵ�ҩ������ÿ��������������������ʹ���IJ��֡�������ָ������Ҫ��Ч��ҩ�����������Ч���á�����������Ч���ⶾ���ߵ�������ǿ�ҵ�ҩЧ�����á���ʹ��������������ã���֤�����е�����ҩ���ܹ�����ݡ�
��һЩ������֤��֧������ԭ���Ϻ���ͨ��ѧ��������ѧ�ҳ��úͳ������쵼�Ķ�������˸�������Ƭ�ijɷ֡�����ҽ�������ư�Ѫ����ҩ���������ۻơ����졢���Ρ����Ƿ����ۻ��е�������������Ա���Ϊ����������������Ѫ��ϸ����Ҫ���������ף�����죬�����е���Ч�ɷ֣����ӡ�ʹ����������������Ѫ��ϸ��������������ͪ����Ϊ������ȥ�����˵��ź�ͨ·����ֹ��Ѫ������ɢ������������ͪ��Ϊ��ʹ��ȥ��ǿϸ������������������롣
ǰ��·����
��ȥ200����ִ�ҽѧ��Ҫ������ֹ�����ƴ�Ⱦ�������Բ��Լ�������ʹ��ȡ�ûԻ͵ijɾ͡���ȶ��ԣ���������������Բ����˻��Լ����Ͻ�չ��������������Щ���������������Ͱ����Ⱥ�Ĭ֢�������������ҽ�Ʊ������õIJ�������������ά�ֵ���Ҫԭ��ͨ������ҽ�������˽⣬�Ƿ��ܹ��Ľ���ҽ����Щ������ϵͳ����������������ϵͳ���ڲ�ʧ�������Ǹ�Ⱦ���µļ����������أ�
�ִ�ҽѧ�������Բ�������ͨ���Dz��ó��ڷ�ҩ�ķ�ʽ�����������³��ڵĶ��Ի��������ԡ���������ڷ�������ʹ��������ɽ���������Ľ�ʹ���߾�������������������������ṩ��һ�����õij�������Ч����Jia˵����Ϊ������һϵ�еijɷ֣�ÿһ����������ɿ���������Ч����ҩ���ֲ�ʹ�����Ƽ���Ч�����ۿۡ����⣬��ҩ�Ƽ�һ����ִ�ҩ��ļ۸���ˡ�������˵��
�в�ҩ������һ��ֵ�ù��Һ��Ļ��Ժ�����Դ�����Ҷ���������������ҩ��ͷ�ǵ�������������й���ҩ��ҵ���ԣ�Ҳ�ǿ�����ҩ������ǰ;����Դ���й�����ǿ��ѧ������ҩ��ҵ�ϵ�Ŭ������Ѱ���ܹ��������������������ܵİ�ȫ��Ч�ĸ������ֵij��Լ����ڴ���ҩ�Ƽ��з��뵥һ����Ч�ɷ֡������ǻ�ԭ�۵����֡����������ֶν������˺��ٵijɹ����ӡ���������űҩ�����غ����ư�Ѫ�������������顣
ֱ��ĿǰΪֹ����û��������ҽ�����з���ҩ��õ�������ŷ���Ͽɡ���ӽ���������sinecatechins��һ���̲���ȡ�ɷֵĻ������࣬������������ֳ�������ࡣSinecatechins����2006������ʳƷ��ҩ���������ͨ���ģ���FDA��һ����Ψһһ��ֲ����ҩ����������ٴ��Ľ������������Ч�ɷֺ����û���δ֪�����������й������ʿ��������������������Ѿ�˳��ͨ���������Ķ����ٴ����鲢��������Ϊ��һ�����ϿɵĴ��й���ͳҽѧ���з�������ֲ����ҩ�
����������ҩ��ܹ���Ǹ�����������ҩ��ķ�ʽ�ƶ��ģ������Dz�����������ҩ������������ʿ�����ŵĸ��ܲ�Henry Sun˵������Ȼ����ҽ��Ҫ�ڿ�ѧ֤�ݵĻ����ϱ�֤���������ǣ�Sun��Ϊ��ѧ���ڼ����Ե�һ���Ƶĵ�һҩ������˿�ѧ����һ����Ҫ����ս�������˵�������IJ�ͬȺ�壬����ͨ���ڵ������ߣ��ı����Ƕ���ҩ��ƫ������
���϶��»������¶��ϣ�
���ٲ�������������֣��������ʹ�л�������Щ�������������ϵ�һ��ͼ�ϵ���ѧ�����ij��֣�Ϊ��ϵͳ����ѧ�ķ�ʽ����ҽѧ�ṩ��һ���µ�;������������ҽ�о�Ա��˵����������ƽ��Zhong Wang��ϵͳ����ѧҲ�������ṩһ����������ѧ����������ҽ��·�ӡ�������ҽ��ϵ���Ҫ�ѵ�������ΰ���ҽ�ľ���۵�ת��Ϊ������ѧ�ҿ�����������ﻯѧ������ѧ�ϵĺ��塣������ Leiden University ��ϵͳ����ѧ��Jan van der Greef˵����ϵͳ����ѧ��һ����������ۺͷ������ߣ��ܹ�����������ϵͳ����
Leroy Hood������ͼϵͳ����ѧ�о�������������������Ϊ���������Ĵ����ˣ�����������ν�ġ�4Pҽ�Ʊ���������Ԥ��predictive, ���廯personalized, Ԥ��preventive�Ͳ��� participatory��Hood��������������ǵ�����ϵͳ����ѧʱ�����µ��ִ�ҽѧ��ʽ��4Pҽѧ��ע�����ͼ����µ��������磬Ȼ��ʶ��������������Ŷ�����������������������뵽��ҽ����ѧ����лϵͳ����ѧ��������ҽѧϵͳ��IJ���խ�ˡ����磬���һЩҽѧ�����ķ�չ�����µı��ͼ���Ӧ����ͬʱ�۲���ʳ��Ķ��ַ�Ӧ��������ն������һ�����ǵġ�����-��֤���о��У����о���Щ�����ǶԵģ���Jia�쵼��С�鶨���ز������ն�������������������ϸ����л���������Ͳ��淴Ӧ�����л����Һ�ɷ֡������Ͳ��Ի���������ͨ����ͬ����ҽ֢�ֵļ������͵IJ��졣��Jia˵������Щ���ᡰ���ҽ�����廯���Ƶ�������Ԥ��ijһ�������һ�ָ�ҩ�����ķ�Ӧ����
���ǰ���Jia�����������ڶ���ʶ��ϵͳ����ѧ�ķ����ͼ����Բ����졣����������Ҫ��չ���������Ƶ�ģ������ģ�ͣ�������л����֮�ࣩ�����磬��������ϸ��ת��Ϊ��ϸ������Jia˵�����ڶ����ǽ���һ���б�Ϊת������ж��λ��Ķ����ҩ��ģ�͡���
�����������
��ѧ�Ŀ������̺Ϳ����ٴ������ȱʧ�谭�˼���������������ͳҽѧ���ִ�ҽѧ�����ϡ����IJ�����������˵�����ƣ�����˵������ħ����ͬʱ����ȱ���������������Ա������۲죨����֮�ࣩ��Ȼ������Щ��������������С��
�������ϵ�ʵʩ���������й��������ڹ���������Ӧ������һ�������Լ���������ҽ��ɫ��Ч�ķ�������Zhimin Wang˵��������ҽ�����������ܵ�;��������Ӧ�����Լ���˼ά����
����ҽ��ϵͳ���������Ӻ��п��ܻ���ʧ����������ϵͳ���ȡ�������Ų���˵�����෴�����ǻ�����䡣��
��ӡ���� �رմ���